Estresse Oxidativo no Autismo: Por Que Medir Apenas Inflamação Não Basta
Estresse Oxidativo no Autismo: Por Que Medir Apenas a Inflamação Não Basta
O ‘Quarteto Diagnóstico’ que revela não apenas o dano celular, mas exatamente onde o sistema de defesa antioxidante falhou — e como intervir com precisão
📅 Publicado em 08 de novembro de 2025
Na medicina moderna, a ligação entre o Transtorno do Espectro Autista (TEA) e o estresse oxidativo é robusta e bem documentada. No entanto, a promessa de tratar o TEA com antioxidantes tem sido frustrantemente inconstante.
Por quê? Porque temos usado as ferramentas erradas.
Por décadas, fomos treinados para usar proxies (substitutos) inflamatórios como evidência de estresse oxidativo. Marcadores como PCR-us elevada, HDL baixo, ou uma Relação Albumina/Globulina diminuída são excelentes para medir inflamação (a “fumaça”).
Mas eles falham em nos dizer três coisas cruciais:
- O “dano” molecular real (a “queimadura”) está ocorrendo?
- Onde, exatamente, o mecanismo de defesa do corpo falhou?
- Como podemos intervir de forma cirúrgica?
Para responder a isso, precisamos de um modelo superior. Não basta procurar a “fumaça”; precisamos encontrar a falha no “sistema anti-incêndio”.
🔥 O Paradigma Quebrado: Medindo “Fumaça” em Vez de “Dano”
O Problema dos Marcadores Tradicionais
Os marcadores inflamatórios convencionais nos dizem que algo está errado, mas não nos dizem o que exatamente está acontecendo no nível molecular.
É como um alarme de incêndio que toca, mas não indica qual andar está pegando fogo, nem se os extintores estão funcionando.
Resultado clínico: Tratamentos antioxidantes genéricos que funcionam para alguns pacientes, mas falham para muitos outros — porque não estamos identificando onde o sistema de defesa antioxidante especificamente colapsou.
A mudança de paradigma necessária:
Em vez de perguntar “Este paciente tem inflamação?”, precisamos perguntar:
- “Há dano molecular mensurável?”
- “Qual linha de defesa antioxidante falhou?”
- “Que cofatores enzimáticos estão depletados?”
Estas perguntas exigem marcadores bioquímicos específicos, não proxies inflamatórios.
🎯 O “Quarteto”: Um Novo Padrão-Ouro para o Diagnóstico Acionável
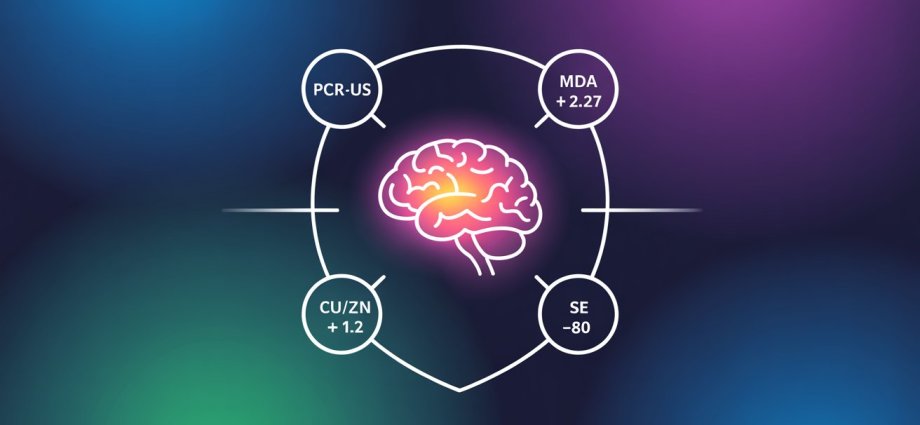
Propomos um painel de quatro marcadores que, juntos, fornecem um diagnóstico inquestionável, medindo a Fonte, o Dano e — o mais importante — as Falhas no Mecanismo de Defesa.
Por que estes 4 marcadores juntos são revolucionários?
Porque pela primeira vez conseguimos não apenas confirmar que há dano oxidativo (MDA), mas também diagnosticar exatamente onde o sistema de defesa falhou (Cu/Zn e Selênio), permitindo intervenções precisas e personalizadas.
Marcador 1: PCR Ultrassensível — A Fonte (O Incêndio)
Este é o nosso ponto de partida. Uma PCR-us > 2,0 mg/L confirma a “Fonte”: um estado inflamatório sistêmico que serve como motor para a produção de espécies reativas de oxigênio (EROs).
Por Que a PCR-us é Importante?
A Proteína C-Reativa ultrassensível é um marcador de fase aguda que reflete atividade inflamatória sistêmica. No contexto do estresse oxidativo:
- Inflamação → Ativação de NADPH oxidase → Produção de superóxido (O₂⁻)
- Quanto maior a inflamação, maior a carga de radicais livres que o sistema antioxidante precisa neutralizar
- A PCR-us elevada nos diz que há um “incêndio ativo” — a máquina está produzindo EROs
⚠️ Atenção Clínica
A PCR-us sozinha NÃO confirma estresse oxidativo. Ela apenas confirma que há inflamação — a “fonte potencial” de radicais livres. Precisamos do MDA para confirmar que o dano está realmente acontecendo.
| Nível de PCR-us | Interpretação | Ação Clínica |
|---|---|---|
| < 1,0 mg/L | Baixo risco inflamatório | Improvável fonte significativa de EROs |
| 1,0 – 2,0 mg/L | Risco intermediário | Monitorar, avaliar outros marcadores |
| > 2,0 mg/L | Inflamação sistêmica confirmada | Fonte ativa de EROs → Prosseguir com MDA |
Marcador 2: Malondialdeído (MDA) — A Prova do Dano Molecular
Este é o marcador de “Dano Consumado”. É a prova da peroxidação lipídica — o dano real às membranas celulares. No entanto, sua medição é um “campo minado” metodológico.
O Paradoxo Laboratorial do MDA
Nossa investigação clínica revelou que laboratórios podem usar métodos contraditórios. Por exemplo:
- Um laudo pode afirmar usar “Espectrofotometria” (confirmado como “TBARS direto”)
- Este é um método inespecífico que mede MDA + “Lixo” (outras substâncias reativas ao ácido tiobarbitúrico)
- Logicamente, este método “sujo” deveria ter valores de referência altos (ex: 5-25 μmol/L)
🚨 O Problema Crítico
Encontramos laudos que usam este mesmo método mas apresentam uma faixa de referência paradoxalmente baixa (ex: 2,5 a 4,0 μmol/L), tornando o resultado não confiável.
Conclusão: Não podemos confiar nos valores de referência fornecidos por laboratórios que usam TBARS sem padronização adequada.
A Solução: O Padrão-Ouro de Altun et al. (2018)
Diante da falta de padronização laboratorial, devemos ignorar os valores de referência do laudo e adotar o padrão-ouro da literatura científica.
Felizmente, o estudo de Altun et al. (2018) fez o trabalho que o laboratório não fez. Eles usaram um método TBARS (o método Ohkawa) e geraram uma curva ROC clinicamente válida a partir de 100 participantes (52 pacientes com TEA, 48 controles saudáveis).
Dados do Estudo Altun et al. (2018):
- Grupo Controle (Saudável): Média de 1,49 μmol/L
- Grupo TEA (Patológico): Média de 4,16 μmol/L
- AUC da Curva ROC: 0,937 (excelente poder discriminatório)
- Corte Clínico Patológico: MDA > 2,27 μmol/L
| Nível de MDA | Interpretação | Significado Clínico |
|---|---|---|
| < 2,27 μmol/L | Faixa normal | Peroxidação lipídica dentro dos limites fisiológicos |
| > 2,27 μmol/L | PATOLÓGICO | Dano oxidativo às membranas celulares CONFIRMADO |
| > 4,0 μmol/L | Altamente patológico | Peroxidação lipídica severa, risco de disfunção celular significativa |
📚 Nota Editorial sobre o Estudo Altun et al. (2018)
O estudo tem um erro de digitação claro, listando a média em “nmol/mL” mas o corte em “mmol/L”. Como 1 nmol/mL = 1 μmol/L, e o corte (2,27) logicamente precisa estar entre a média do controle (1,49) e a média do TEA (4,16), o corte correto é 2,27 μmol/L.
Marcador 3: Relação Cobre/Zinco (Cu/Zn) — Falha na 1ª Frente de Defesa
Ter MDA alto é o dano. Agora, precisamos saber por que as defesas falharam. O corpo tem duas etapas principais de defesa enzimática, e a primeira delas depende da enzima SOD1 (Superóxido Dismutase 1).
Como Funciona a 1ª Linha de Defesa?
A enzima SOD1 é a linha de frente. Ela neutraliza o radical superóxido (O₂⁻) antes que ele cause dano. Para funcionar, a SOD1 precisa de dois cofatores metálicos:
- Zinco (Zn): O “freio” do sistema. Essencial para a atividade da SOD1.
- Cobre (Cu): O “acelerador” do dano. Pró-oxidante que catalisa a Reação de Fenton, criando o radical hidroxila (·OH), um dos mais destrutivos.
Analogia Clínica:
Uma Relação Cu/Zn elevada (Cobre Alto / Zinco Baixo) significa que o paciente está “sem freio e com o acelerador no fundo”.
- Zinco insuficiente → SOD1 não funciona adequadamente → Superóxido se acumula
- Cobre em excesso → Reação de Fenton intensificada → Produção de radicais hidroxila
Interpretação Clínica
| Relação Cu/Zn | Interpretação | Estado da SOD1 |
|---|---|---|
| < 1,0 | Ideal | SOD1 bem suprida, defesa antioxidante funcional |
| 1,0 – 1,2 | Limítrofe | Risco de insuficiência da SOD1 em situações de estresse |
| > 1,2 | PATOLÓGICO | Falha na 1ª frente: SOD1 deficiente em Zinco |
💡 Implicação Terapêutica
Um paciente com MDA alto + Relação Cu/Zn > 1,2 tem diagnóstico preciso:
- ✅ Confirmação de dano oxidativo (MDA)
- ✅ Identificação da falha específica (SOD1 deficiente em Zinco)
- ✅ Intervenção direcionada: Suplementação de Zinco
Isso é diagnóstico de precisão acionável.
Marcador 4: Selênio Sérico — Falha na 2ª Frente de Defesa
A SOD1 (1ª Frente) neutraliza o superóxido (O₂⁻) transformando-o em peróxido de hidrogênio (H₂O₂). Mas o H₂O₂ também é reativo e precisa ser neutralizado. A 2ª Frente é a enzima Glutationa Peroxidase (GPx), e seu cofator indispensável é o Selênio (Se).
A Guerra de Duas Frentes
Um paciente pode ter uma SOD1 perfeita (Cu/Zn normal), mas se lhe faltar Selênio, o H₂O₂ se acumula e o sistema falha de qualquer forma.
Sequência da Defesa Antioxidante:
- 1ª Frente (SOD1): O₂⁻ + O₂⁻ → H₂O₂ + O₂ (requer Zinco)
- 2ª Frente (GPx): H₂O₂ → H₂O + O₂ (requer Selênio)
Se qualquer uma das duas frentes falha, o paciente fica vulnerável ao dano oxidativo.
Níveis de Selênio e Atividade da GPx
| Selênio Sérico | Status | Atividade da GPx |
|---|---|---|
| > 100 μg/L | Adequado | GPx com atividade máxima |
| 80 – 100 μg/L | Limítrofe | GPx funcionando, mas não em capacidade plena |
| < 80 μg/L | INSUFICIENTE | Falha na 2ª frente: GPx não atinge atividade máxima |
🎯 Cenários Clínicos Possíveis
Cenário 1: MDA alto + Cu/Zn > 1,2 + Selênio < 80 μg/L
- Diagnóstico: Falha em AMBAS as frentes de defesa
- Intervenção: Zinco + Selênio
Cenário 2: MDA alto + Cu/Zn normal + Selênio < 80 μg/L
- Diagnóstico: 1ª frente OK, mas falha na 2ª frente
- Intervenção: Selênio (Zinco não é necessário)
Cenário 3: MDA alto + Cu/Zn > 1,2 + Selênio normal
- Diagnóstico: Falha apenas na 1ª frente
- Intervenção: Zinco (Selênio não é necessário)
🧩 A Conexão com o Autismo: Do Diagnóstico ao Tratamento
Este “Quarteto” não é apenas diagnóstico; ele é acionável. Ele nos diz exatamente como intervir no paciente com TEA.
O estudo de Altun et al. (2018) nos dá a pista final. Ele não encontrou apenas MDA alto; ele encontrou níveis significativamente mais altos de:
- SOD: 295 U/mL no grupo TEA vs. 109 U/mL no controle
- Catalase: 184 U/mL no grupo TEA vs. 72 U/mL no controle
🔬 Interpretação Científica Crítica
O sistema de defesa antioxidante do paciente com TEA não está “preguiçoso”. Ele está em “resposta compensatória”.
É um exército sobrecarregado, lutando uma batalha desesperada e “acelerando ao máximo” (aumentando as enzimas).
Mas este exército está ficando sem munição:
- A SOD (1ª Frente) está alta, consumindo Zinco
- A GPx (2ª Frente) está ativa, consumindo Selênio
Por Que Antioxidantes Genéricos Falham
É por isso que o tratamento antioxidante “padrão” (como Vitamina C ou E) falha em muitos casos. Ele envia “bombeiros externos” (antioxidantes) quando o que o exército do corpo realmente precisa é de “munição” (Zinco e Selênio) para que suas próprias enzimas (SOD e GPx) possam vencer a guerra.
⚠️ Correlação Clínica Importante
O estudo de Altun (2018) fecha o ciclo ao provar que o dano não é um achado incidental: os níveis de MDA têm correlação positiva com a gravidade dos sintomas do autismo (a pontuação CARS).
Ou seja: quanto maior o dano oxidativo, mais severos os sintomas. Isso valida a importância clínica de medir e tratar o estresse oxidativo de forma precisa.
IA no Diagnóstico de Precisão do Estresse Oxidativo
A Inteligência Artificial está transformando como interpretamos e agimos sobre o “Quarteto Diagnóstico”, elevando o diagnóstico de precisão a um novo patamar.
🔍 IA na Interpretação Laboratorial
Algoritmos de machine learning podem identificar padrões complexos entre os 4 marcadores que não são óbvios à análise humana.
Exemplo prático: Um sistema de IA pode detectar que pacientes com MDA entre 2,3-2,8 μmol/L + Cu/Zn > 1,3 + Selênio 75-85 μg/L têm 87% de probabilidade de resposta positiva à suplementação combinada (Zn + Se), enquanto aqueles com apenas Cu/Zn alterado respondem melhor ao Zinco isolado.
Esses padrões sutis de “assinatura bioquímica” são difíceis de capturar manualmente, mas a IA os identifica analisando centenas de casos.
🎯 IA na Personalização Terapêutica
Modelos preditivos baseados em IA podem prever a resposta terapêutica individual antes mesmo de iniciar o tratamento.
Como funciona: Ao inserir os valores do Quarteto + dados clínicos (idade, peso, comorbidades, uso de medicações), a IA calcula:
- Probabilidade de resposta clínica em 3, 6 e 12 meses
- Dose otimizada de Zinco e Selênio para aquele paciente específico
- Risco de não-resposta ou necessidade de ajustes
Isso transforma “tentativa e erro” em medicina de precisão orientada por dados.
📊 IA no Monitoramento Longitudinal
Sistemas inteligentes podem acompanhar a evolução temporal dos 4 marcadores e alertar precocemente sobre deterioração ou necessidade de ajuste.
Funcionalidade prática:
- Detecção de tendências (ex: MDA subindo apesar do tratamento)
- Alertas automáticos quando qualquer marcador sai da faixa-alvo
- Sugestões de reavaliação baseadas em desvios do padrão esperado
Em vez de esperar uma consulta de rotina, o médico é notificado proativamente quando há sinais de problema.
💡 O Futuro do Diagnóstico de Precisão
A combinação do “Quarteto Diagnóstico” (bioquímica precisa) com IA (análise de padrões complexos) representa o futuro da medicina personalizada em TEA.
Não estamos mais limitados a protocolos genéricos. Podemos agora:
- ✅ Diagnosticar com precisão molecular
- ✅ Identificar exatamente onde o sistema falhou
- ✅ Prever resposta terapêutica individual
- ✅ Monitorar proativamente a evolução
- ✅ Ajustar tratamento baseado em dados reais
Isso é o que chamamos de Medicina 5.0: humana, precisa e inteligente.
📋 Protocolo Clínico Prático: Implementação do Quarteto
Fluxograma de Avaliação Diagnóstica
PASSO 1: Confirmação da Fonte (Inflamação)
- Solicitar: PCR-us
- Se PCR-us > 2,0 mg/L → Prosseguir para Passo 2
- Se PCR-us < 2,0 mg/L → Fonte inflamatória improvável, considerar outras causas para sintomas
PASSO 2: Confirmação do Dano (Peroxidação Lipídica)
- Solicitar: Malondialdeído (MDA)
- CRÍTICO: Ignorar valor de referência do laboratório
- Usar corte de Altun et al. (2018): MDA > 2,27 μmol/L = PATOLÓGICO
- Se MDA > 2,27 μmol/L → Dano oxidativo CONFIRMADO → Prosseguir para Passo 3
PASSO 3: Identificação das Falhas na Defesa
- Solicitar: Cobre sérico + Zinco sérico (calcular relação Cu/Zn)
- Solicitar: Selênio sérico
Interpretação:
- Cu/Zn > 1,2 = Falha na 1ª frente (SOD1)
- Selênio < 80 μg/L = Falha na 2ª frente (GPx)
PASSO 4: Intervenção Direcionada
| Achado | Intervenção |
| Cu/Zn > 1,2 + Selênio < 80 | Zinco + Selênio |
| Cu/Zn > 1,2 + Selênio normal | Zinco isolado |
| Cu/Zn normal + Selênio < 80 | Selênio isolado |
⚠️ Considerações Importantes
- Não prescreva antioxidantes genéricos sem primeiro identificar quais cofatores enzimáticos estão deficientes
- Reavalie o Quarteto após 3-6 meses de suplementação para verificar resposta
- Correlacione melhora bioquímica com melhora clínica (escalas comportamentais, CARS, etc.)
- Ajuste doses conforme evolução dos marcadores, não de forma empírica
🎯 Transforme Seu Diagnóstico em Ação
O “Quarteto Diagnóstico” está disponível em laboratórios de análises clínicas no Brasil.
Medir não basta. Precisamos medir o que importa — e agir com precisão.
✅ Conclusão: O Novo Mandato Clínico
O estresse oxidativo no TEA não é mais uma “caixa preta”. Não podemos mais nos contentar com laudos de MDA não padronizados ou diagnósticos baseados apenas em inflamação.
O “Quarteto” (PCR-us, Relação Cu/Zn, Selênio Sérico e MDA > 2,27 μmol/L) tem potencial para ser o novo padrão-ouro. Ele nos permite identificar se o paciente está oxidado, onde sua defesa falhou e exatamente como vamos intervir — não com suposições, mas com precisão bioquímica.
Este é o mandato clínico da medicina moderna: diagnóstico molecular preciso, intervenção direcionada e monitoramento baseado em evidências.
A tecnologia está disponível. A ciência está validada. O próximo passo depende de nós, clínicos, aplicarmos este conhecimento na prática diária.
📚 Referência Principal
Altun H, Şahin N, Kurutaş EB, Karaaslan U, Sevgen FH, Fındıklı E. Assessment of malondialdehyde levels, superoxide dismutase, and catalase activity in children with autism spectrum disorders. Psychiatry Clin Psychopharmacol. 2018;28(4):408-415. doi:10.1080/24750573.2018.1470360
Disponível em: https://doi.org/10.1080/24750573.2018.1470360
Nota: Este estudo forneceu os dados de MDA (média controle: 1,49 nmol/mL, média TEA: 4,16 nmol/mL, corte patológico: 2,27 mmol/L [corrigido para μmol/L conforme análise metodológica], AUC 0,937) e os níveis de SOD e Catalase citados neste editorial.
Oxidative Stress in Autism: Why Measuring Only Inflammation Is Not Enough
The ‘Diagnostic Quartet’ that reveals not only cellular damage, but exactly where the antioxidant defense system failed — and how to intervene with precision
📅 Published on November 08, 2025
In modern medicine, the link between Autism Spectrum Disorder (ASD) and oxidative stress is robust and well documented. However, the promise of treating ASD with antioxidants has been frustratingly inconsistent.
Why? Because we have been using the wrong tools.
For decades, we have been trained to use inflammatory proxies (substitutes) as evidence of oxidative stress. Markers such as elevated hs-CRP, low HDL, or a decreased Albumin/Globulin Ratio are excellent for measuring inflammation (the “smoke”).
But they fail to tell us three crucial things:
- Is the real molecular “damage” (the “burn”) occurring?
- Where, exactly, did the body’s defense mechanism fail?
- How can we intervene in a surgical manner?
To answer this, we need a superior model. It is not enough to look for “smoke”; we need to find the failure in the “fire suppression system.”
🔥 The Broken Paradigm: Measuring “Smoke” Instead of “Damage”
The Problem with Traditional Markers
Conventional inflammatory markers tell us that something is wrong, but they don’t tell us what exactly is happening at the molecular level.
It’s like a fire alarm that rings but doesn’t indicate which floor is on fire, nor whether the extinguishers are working.
Clinical outcome: Generic antioxidant treatments that work for some patients but fail for many others — because we are not identifying where the antioxidant defense system specifically collapsed.
The necessary paradigm shift:
Instead of asking “Does this patient have inflammation?”, we need to ask:
- “Is there measurable molecular damage?”
- “Which line of antioxidant defense failed?”
- “Which enzymatic cofactors are depleted?”
These questions require specific biochemical markers, not inflammatory proxies.
🎯 The “Quartet”: A New Gold Standard for Actionable Diagnosis
We propose a panel of four markers that, together, provide an unquestionable diagnosis, measuring the Source, the Damage, and — most importantly — the Failures in the Defense Mechanism.
Why are these 4 markers together revolutionary?
Because for the first time we can not only confirm that there is oxidative damage (MDA), but also diagnose exactly where the defense system failed (Cu/Zn and Selenium), allowing for precise and personalized interventions.
Marker 1: High-Sensitivity CRP — The Source (The Fire)
This is our starting point. An hs-CRP > 2.0 mg/L confirms the “Source”: a systemic inflammatory state that serves as the engine for the production of reactive oxygen species (ROS).
Why Is hs-CRP Important?
High-sensitivity C-Reactive Protein is an acute-phase marker that reflects systemic inflammatory activity. In the context of oxidative stress:
- Inflammation → NADPH oxidase activation → Superoxide production (O₂⁻)
- The greater the inflammation, the greater the load of free radicals that the antioxidant system needs to neutralize
- Elevated hs-CRP tells us there is an “active fire” — the machine is producing ROS
⚠️ Clinical Caution
hs-CRP alone does NOT confirm oxidative stress. It only confirms that there is inflammation — the “potential source” of free radicals. We need MDA to confirm that damage is actually happening.
| hs-CRP Level | Interpretation | Clinical Action |
|---|---|---|
| < 1.0 mg/L | Low inflammatory risk | Unlikely significant ROS source |
| 1.0 – 2.0 mg/L | Intermediate risk | Monitor, evaluate other markers |
| > 2.0 mg/L | Confirmed systemic inflammation | Active ROS source → Proceed to MDA |
Marker 2: Malondialdehyde (MDA) — Proof of Molecular Damage
This is the “Accomplished Damage” marker. It is proof of lipid peroxidation — the actual damage to cell membranes. However, its measurement is a methodological “minefield.”
The Laboratory Paradox of MDA
Our clinical investigation revealed that laboratories may use contradictory methods. For example:
- A report may claim to use “Spectrophotometry” (confirmed as “direct TBARS”)
- This is a non-specific method that measures MDA + “Junk” (other substances reactive to thiobarbituric acid)
- Logically, this “dirty” method should have high reference values (e.g., 5-25 μmol/L)
🚨 The Critical Problem
We found reports that use this same method but present a paradoxically low reference range (e.g., 2.5 to 4.0 μmol/L), making the result unreliable.
Conclusion: We cannot trust the reference values provided by laboratories that use TBARS without proper standardization.
The Solution: The Gold Standard from Altun et al. (2018)
Given the lack of laboratory standardization, we must ignore the reference values from the report and adopt the gold standard from the scientific literature.
Fortunately, the study by Altun et al. (2018) did the work that the laboratory did not. They used a TBARS method (the Ohkawa method) and generated a clinically valid ROC curve from 100 participants (52 patients with ASD, 48 healthy controls).
Data from the Altun et al. (2018) Study:
- Control Group (Healthy): Mean of 1.49 μmol/L
- ASD Group (Pathological): Mean of 4.16 μmol/L
- ROC Curve AUC: 0.937 (excellent discriminatory power)
- Clinical Pathological Cutoff: MDA > 2.27 μmol/L
| MDA Level | Interpretation | Clinical Significance |
|---|---|---|
| < 2.27 μmol/L | Normal range | Lipid peroxidation within physiological limits |
| > 2.27 μmol/L | PATHOLOGICAL | Oxidative damage to cell membranes CONFIRMED |
| > 4.0 μmol/L | Highly pathological | Severe lipid peroxidation, risk of significant cellular dysfunction |
📚 Editorial Note on the Altun et al. (2018) Study
The study has a clear typographical error, listing the mean in “nmol/mL” but the cutoff in “mmol/L”. Since 1 nmol/mL = 1 μmol/L, and the cutoff (2.27) logically needs to be between the control mean (1.49) and the ASD mean (4.16), the correct cutoff is 2.27 μmol/L.
Marker 3: Copper/Zinc Ratio (Cu/Zn) — Failure at the 1st Defense Line
Having high MDA is the damage. Now, we need to know why the defenses failed. The body has two main stages of enzymatic defense, and the first one depends on the SOD1 enzyme (Superoxide Dismutase 1).
How Does the 1st Line of Defense Work?
The SOD1 enzyme is the front line. It neutralizes the superoxide radical (O₂⁻) before it causes damage. To function, SOD1 needs two metal cofactors:
- Zinc (Zn): The “brake” of the system. Essential for SOD1 activity.
- Copper (Cu): The “accelerator” of damage. A pro-oxidant that catalyzes the Fenton Reaction, creating the hydroxyl radical (·OH), one of the most destructive.
Clinical Analogy:
An elevated Cu/Zn Ratio (High Copper / Low Zinc) means the patient is “without brakes and with the accelerator to the floor”.
- Insufficient zinc → SOD1 does not work properly → Superoxide accumulates
- Excess copper → Intensified Fenton Reaction → Production of hydroxyl radicals
Clinical Interpretation
| Cu/Zn Ratio | Interpretation | SOD1 Status |
|---|---|---|
| < 1.0 | Ideal | SOD1 well supplied, functional antioxidant defense |
| 1.0 – 1.2 | Borderline | Risk of SOD1 insufficiency in stress situations |
| > 1.2 | PATHOLOGICAL | Failure at the 1st line: SOD1 deficient in Zinc |
💡 Therapeutic Implication
A patient with high MDA + Cu/Zn Ratio > 1.2 has a precise diagnosis:
- ✅ Confirmation of oxidative damage (MDA)
- ✅ Identification of the specific failure (SOD1 deficient in Zinc)
- ✅ Targeted intervention: Zinc Supplementation
This is actionable precision diagnosis.
Marker 4: Serum Selenium — Failure at the 2nd Defense Line
SOD1 (1st Line) neutralizes superoxide (O₂⁻) by transforming it into hydrogen peroxide (H₂O₂). But H₂O₂ is also reactive and needs to be neutralized. The 2nd Line is the Glutathione Peroxidase (GPx) enzyme, and its indispensable cofactor is Selenium (Se).
The Two-Front War
A patient may have perfect SOD1 (normal Cu/Zn), but if they lack Selenium, H₂O₂ accumulates and the system fails anyway.
Antioxidant Defense Sequence:
- 1st Line (SOD1): O₂⁻ + O₂⁻ → H₂O₂ + O₂ (requires Zinc)
- 2nd Line (GPx): H₂O₂ → H₂O + O₂ (requires Selenium)
If either line fails, the patient is vulnerable to oxidative damage.
Selenium Levels and GPx Activity
| Serum Selenium | Status | GPx Activity |
|---|---|---|
| > 100 μg/L | Adequate | GPx with maximum activity |
| 80 – 100 μg/L | Borderline | GPx functioning but not at full capacity |
| < 80 μg/L | INSUFFICIENT | Failure at the 2nd line: GPx does not reach maximum activity |
🎯 Possible Clinical Scenarios
Scenario 1: High MDA + Cu/Zn > 1.2 + Selenium < 80 μg/L
- Diagnosis: Failure at BOTH defense lines
- Intervention: Zinc + Selenium
Scenario 2: High MDA + Normal Cu/Zn + Selenium < 80 μg/L
- Diagnosis: 1st line OK, but failure at the 2nd line
- Intervention: Selenium (Zinc is not necessary)
Scenario 3: High MDA + Cu/Zn > 1.2 + Normal Selenium
- Diagnosis: Failure only at the 1st line
- Intervention: Zinc (Selenium is not necessary)
🧩 The Connection with Autism: From Diagnosis to Treatment
This “Quartet” is not just diagnostic; it is actionable. It tells us exactly how to intervene in patients with ASD.
The study by Altun et al. (2018) gives us the final clue. It did not only find high MDA; it found significantly higher levels of:
- SOD: 295 U/mL in the ASD group vs. 109 U/mL in controls
- Catalase: 184 U/mL in the ASD group vs. 72 U/mL in controls
🔬 Critical Scientific Interpretation
The antioxidant defense system in patients with ASD is not “lazy”. It is in “compensatory response”.
It is an overworked army, fighting a desperate battle and “accelerating to the max” (increasing enzymes).
But this army is running out of ammunition:
- SOD (1st Line) is high, consuming Zinc
- GPx (2nd Line) is active, consuming Selenium
Why Generic Antioxidants Fail
This is why “standard” antioxidant treatment (such as Vitamin C or E) fails in many cases. It sends “external firefighters” (antioxidants) when what the body’s army really needs is “ammunition” (Zinc and Selenium) so that its own enzymes (SOD and GPx) can win the war.
⚠️ Important Clinical Correlation
The study by Altun (2018) closes the loop by proving that the damage is not an incidental finding: MDA levels have a positive correlation with the severity of autism symptoms (CARS score).
In other words: the greater the oxidative damage, the more severe the symptoms. This validates the clinical importance of measuring and treating oxidative stress precisely.
AI in Precision Diagnosis of Oxidative Stress
Artificial Intelligence is transforming how we interpret and act on the “Diagnostic Quartet,” elevating precision diagnosis to a new level.
🔍 AI in Laboratory Interpretation
Machine learning algorithms can identify complex patterns among the 4 markers that are not obvious to human analysis.
Practical example: An AI system can detect that patients with MDA between 2.3-2.8 μmol/L + Cu/Zn > 1.3 + Selenium 75-85 μg/L have an 87% probability of positive response to combined supplementation (Zn + Se), while those with only altered Cu/Zn respond better to Zinc alone.
These subtle patterns of “biochemical signature” are difficult to capture manually, but AI identifies them by analyzing hundreds of cases.
🎯 AI in Therapeutic Personalization
Predictive models based on AI can predict individual therapeutic response before even starting treatment.
How it works: By entering the Quartet values + clinical data (age, weight, comorbidities, medication use), AI calculates:
- Probability of clinical response at 3, 6, and 12 months
- Optimized dose of Zinc and Selenium for that specific patient
- Risk of non-response or need for adjustments
This transforms “trial and error” into data-driven precision medicine.
📊 AI in Longitudinal Monitoring
Intelligent systems can track the temporal evolution of the 4 markers and alert early about deterioration or need for adjustment.
Practical functionality:
- Detection of trends (e.g., MDA rising despite treatment)
- Automatic alerts when any marker goes out of target range
- Re-evaluation suggestions based on deviations from expected pattern
Instead of waiting for a routine appointment, the physician is notified proactively when there are signs of problems.
💡 The Future of Precision Diagnosis
The combination of the “Diagnostic Quartet” (precise biochemistry) with AI (complex pattern analysis) represents the future of personalized medicine in ASD.
We are no longer limited to generic protocols. We can now:
- ✅ Diagnose with molecular precision
- ✅ Identify exactly where the system failed
- ✅ Predict individual therapeutic response
- ✅ Proactively monitor evolution
- ✅ Adjust treatment based on real data
This is what we call Medicine 5.0: human, precise, and intelligent.
📋 Practical Clinical Protocol: Implementing the Quartet
Diagnostic Evaluation Flowchart
STEP 1: Confirmation of the Source (Inflammation)
- Order: hs-CRP
- If hs-CRP > 2.0 mg/L → Proceed to Step 2
- If hs-CRP < 2.0 mg/L → Inflammatory source unlikely, consider other causes for symptoms
STEP 2: Confirmation of Damage (Lipid Peroxidation)
- Order: Malondialdehyde (MDA)
- CRITICAL: Ignore laboratory reference value
- Use Altun et al. (2018) cutoff: MDA > 2.27 μmol/L = PATHOLOGICAL
- If MDA > 2.27 μmol/L → Oxidative damage CONFIRMED → Proceed to Step 3
STEP 3: Identification of Defense Failures
- Order: Serum Copper + Serum Zinc (calculate Cu/Zn ratio)
- Order: Serum Selenium
Interpretation:
- Cu/Zn > 1.2 = Failure at the 1st line (SOD1)
- Selenium < 80 μg/L = Failure at the 2nd line (GPx)
STEP 4: Targeted Intervention
| Finding | Intervention |
| Cu/Zn > 1.2 + Selenium < 80 | Zinc + Selenium |
| Cu/Zn > 1.2 + Normal Selenium | Zinc alone |
| Normal Cu/Zn + Selenium < 80 | Selenium alone |
⚠️ Important Considerations
- Do not prescribe generic antioxidants without first identifying which enzymatic cofactors are deficient
- Re-evaluate the Quartet after 3-6 months of supplementation to verify response
- Correlate biochemical improvement with clinical improvement (behavioral scales, CARS, etc.)
- Adjust doses according to marker evolution, not empirically
🎯 Transform Your Diagnosis into Action
The “Diagnostic Quartet” is available in clinical analysis laboratories. Don’t wait any longer to offer precision diagnosis to your patients with ASD.
Measuring is not enough. We need to measure what matters — and act with precision.
✅ Conclusion: The New Clinical Mandate
Oxidative stress in ASD is no longer a “black box.” We can no longer settle for non-standardized MDA reports or diagnoses based only on inflammation.
The “Quartet” (hs-CRP, Cu/Zn Ratio, Serum Selenium, and MDA > 2.27 μmol/L) is the new gold standard. It allows us to identify if the patient is oxidized, where their defense failed, and exactly how we will intervene — not with assumptions, but with biochemical precision.
This is the mandate of modern medicine: precise molecular diagnosis, targeted intervention, and evidence-based monitoring.
The technology is available. The science is validated. The next step depends on us, clinicians, to apply this knowledge in daily practice.
📚 Main Reference
Altun H, Şahin N, Kurutaş EB, Karaaslan U, Sevgen FH, Fındıklı E. Assessment of malondialdehyde levels, superoxide dismutase, and catalase activity in children with autism spectrum disorders. Psychiatry Clin Psychopharmacol. 2018;28(4):408-415. doi:10.1080/24750573.2018.1470360
Available at: https://doi.org/10.1080/24750573.2018.1470360
Note: This study provided the MDA data (control mean: 1.49 nmol/mL, ASD mean: 4.16 nmol/mL, pathological cutoff: 2.27 mmol/L [corrected to μmol/L based on methodological analysis], AUC 0.937) and the SOD and Catalase levels cited in this editorial.